
In recent years the gastric sleeve has quickly become the most popular surgical weight loss procedure in the UK and throughout the world. For example, in the US between 2010-2013, the sleeve increased from 9% of all procedures to almost 50%. As will be made clear below, the sleeve has obvious advantages, but it also has some disadvantages which you should be aware of.
So, let’s first have a brief look at what a sleeve gastrectomy involves.
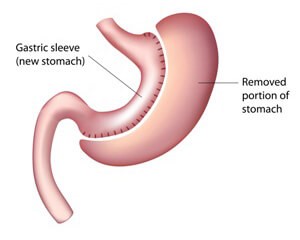
As can be seen from the image opposite, the operation requires complete removal of around 80% of the body of the stomach. This is done using a special instrument which cuts and staples at the same time. What remains of the stomach has the appearance of a sleeve – or perhaps more accurately a banana. This is done under a general anaesthetic using keyhole surgery and takes around 1-1.5 hours to complete.
A key advantage is that, unlike gastric bypass, with a sleeve gastrectomy the food you eat enters and leaves the stomach in the same way it did before surgery.
From start to finish the staff were amazing and so reassuring. Had a gastric band fitted in March 2021 and honestly I’m sorry I didn’t do it years ago. Read More
I felt very informed and safe and well looked after. I had a breast augmentation in June 2018 and couldn’t be happier from start to finish. Read More
Couldn’t have dreamed of a better experience! Made me so comfortable and at ease. Couldn’t recommend Auralia enough I have never ever been happier! Read More
I couldn’t be happier with how my surgery went and I wouldn’t recommend anyone else I choose Auralia because of how helpful and friendly every single member of their team was to me. I couldn’t be happier with how my surgery went and I wouldn’t recommend anyone else! Read More
Not only life-changing has given me a newfound confidence in myself. I had two surgeries with the clinic. And everything from consultation, pre-op and post-op care was amazing. Read More
I couldn't be more pleased from my first consultation. I had a tummy tuck with muscle repair 8 weeks ago now and I couldn't be more pleased from my first consultation. Read More
Weight loss after a sleeve is achieved in two ways.
Another result of these hormonal changes is that diabetic control can start to improve even before you lose weight.
Aside from the two main mechanisms Another feature of the sleeve is that patients report changes in food preferences, with a reduced interest in sweets, high fat foods and alcoholic drinks, though whether these changes are sustained in the longer-term is not clear.
As with any bariatric procedure, the sleeve has important health benefits, these are:
Initial weight loss with a sleeve is high – in some studies as high as 75% of excess weight. This is one of the reasons why the sleeve has become so popular; it appears to offer dramatic weight loss relatively easily and, unlike the gastric band, it seems to require minimal follow-up. However, the longer-term results are not quite so optimistic.
Despite the dramatic early weight loss, longer-term results with the sleeve show a pattern of weight regain over time.
For example, in one study, excess weight loss at 1-year was 71% but fell to 53% at 10-years. In another published trial, excess weight loss at 1, 3,5 and 8-years, was 72, 86, 63 and 52%.
Why does this weight regain occur? It’s probably a combination of stretching of the gastric remnant (the 20% of stomach that remains after surgery), poor dietary habits and a return of the appetite due to increasing ghrelin levels.
The sleeve gastrectomy is the riskiest of the available surgical weight loss procedures.
The three main risks (two post-surgical and the third a later complication) are as follows:
There is a widespread perception that the sleeve is a quicker, easier and more effective option than a gastric band. There is some truth in this, because (unlike the band) the sleeve does not require regular adjustment and (unlike the gastric bypass) it does not involve cutting the bowel. There is no doubt that for many individuals the sleeve is a good option, but it’s important to be fully aware of the risks and benefits.
In recent years there has been a 4-fold increase in the number of patients in the UK undergoing sleeve gastrectomy. This trend mirrors what is happening in other countries, notably the US where the proportion of sleeve gastrectomy procedures increased from 9.3% in 2010 to 49% in 2013. There are a number of reasons for the growing popularity of the sleeve, the most obvious being that it is an effective procedure for many patients considering a surgical weight loss procedure. In general, we believe the sleeve becomes an option for younger people when the body mass index (BMI) exceeds 40kg/m2 or greater.
However, experience suggests there are some common and important misconceptions about the risks and benefits of the sleeve versus the gastric band, which you need to consider carefully.
| Common misconceptions regarding sleeve gastrectomy (SG) | The evidence |
| Weight loss with the sleeve is inevitably greater than that achieved with LAGB. | It’s true that initial weight loss with the sleeve tends to be greater than with the band, mainly because the sleeve actually reduces the level of a hormone called ghrelin. Ghrelin is sometimes called the “hunger hormone” because it stimulates appetite, increases food intake and promotes fat storage.However, emerging evidence suggests that this initial advantage of the sleeve over the band may not be maintained. A number of recent studies have shown that weight regain with the sleeve is quite common, so that after 5-years there may be little, if any, difference in weight loss between the two procedures.
There is also evidence to show that the more gradual weight loss with the gastric band, may help to preserve a much greater proportion of muscle mass than with operations such as gastric bypass or sleeve gastrectomy. This selective preservation of muscle tissue with the band, may help to maintain weight loss in the longer term. |
| You don’t have to work as hard as you do with the gastric band. | Because of the impact of the sleeve on appetite hormones such as ghrelin, initial weight loss after a sleeve may seem more easily achieved than with a gastric band. However, all surgical weight loss procedures require substantial and sustained changes in lifestyle if long-term success is to be achieved – and the sleeve is no exception to this. The erroneous perception on the part of the patient that the sleeve is an easy weight loss option, is a key factor in the eventual failure of the procedure. Quite simply, you get out of the procedure what you put in! |
| You may have heard people say that SG is as effective as a gastric bypass, but is as safe to perform as a gastric band. | This is simply not true. Because the sleeve and gastric bypass involving amputation and/or stapling of the stomach and bowel, they carry a significantly higher risk than implantation of a gastric band. There is no doubt at all that the band is the safest of all the currently available surgical weight loss procedures. |
| I have been told that the risk of a leak with a sleeve gastrectomy, whilst potentially serious, is actually very low. | A leak consists of gastric (stomach) fluids leaking out at the staple line. It is a very serious and potentially life-threatening complication. Nowadays, in expert hands the risk of a leak is probably no more than around 1%, though it can be much higher than this. Thus whilst infrequent, a leak is by no means rareMoreover, if a leak does occur, it may require treatment in an intensive care unit (ICU) for an extended period of time. |
| Longer term complications are much more frequent with the gastric band than with SG. | A re-operation may be necessary with any type of weight loss surgery. In published studies, the sleeve gastrectomy has a complication rate identical to that of the gastric band (13%) and a similar re-operation rate (12% vs 9%)5. At Healthier Weight our 3-year gastric band re-operation rate is just 4%.It should also be borne in mind that complications following LSG tend to be much more serious than those after LAGB. |
| Compared with the gastric band, there are far fewer things that can go wrong with the sleeve in the long-term | It is true that the gastric band has a number of potential complications, such as slippage and port/tubing complications, which do not occur with the sleeve. However, both the band and the sleeve can fail because of poor eating habits in which the pouch (in the case of the band) or the gastric remnant (in the case of the sleeve) can stretch. This means that patients start eating large portions again and (inevitably) putting on weight.However, the sleeve has another complication which can cause significant problems post-surgery. This is called gastro-oesophageal reflux disease (GORD), more commonly known as heartburn. Reflux is actually quite common in patients undergoing weight-loss surgery, but whereas the gastric band actually improves reflux, a sleeve can sometimes make it considerably worse. Moreover, a significant proportion of patients (around 9%) who did not have reflux prior to the procedure, will develop this as a direct result of the surgery.
It is not entirely clear what the significance of this increased risk of reflux after LSG might be, because we do not yet have long-term results (>10-years) for the procedure. However, it is clearly not a trivial issue and it is certainly something to be taken into account, especially if you have a prior history of GORD. In fact, if you have been taking medication for reflux for any length of time, we may well advise you against having a sleeve gastrectomy. |
| I have type 2 diabetes and I’m much more likely to get rid of it with a sleeve gastrectomy than a gastric band. | It is true that the LSG has a greater impact on type 2 diabetes than the gastric band and it appears to exert its effects independently of weight loss. This is because the sleeve has a direct impact on the hormones involved in glucose (sugar) metabolism, which the band does not. However, there is emerging evidence to suggest that although LSG has a large effect initially, the long-term benefits of the sleeve on diabetes seem to diminish. A recent study showed that remission of type 2 diabetes in LSG patients was found in 50.7% of patients at Year 1, 38% in at Year 3 and just 20% at Year 5.It’s also important to note that although the band may not be as powerful as the sleeve in the initial stages, it can still have a very positive impact on diabetes. |
| Sleeve gastrectomy is a permanent weight loss solution | All bariatric procedures potentially provide a permanent weight loss solution. However, the sleeve gastrectomy involves amputating around 85% of your stomach, whereas gastric band is fully reversible. In this sense the sleeve is permanent, but this does not necessarily mean that the weight loss is permanent. Most importantly, however, the gastric band is completely reversible and leaves all other surgical options open. |
Aside from the general eligibility criteria (see here), the qualifying criteria for a sleeve are as below:
| Advantages | Disadvantages |
| Excellent initial weight loss | Risk of leak and bleeding – sleeve is the riskiest procedure |
| Does not require frequent clinic attendance for adjustments | Tendency to weight regain in longer term |
| Reduces hunger hormones (unlike the gastric band) | Increased risk of reflux post-surgery |
| Preservation of normal passage of food through the stomach (unlike gastric bypass) | Need for long-term vitamin and mineral Supplementation to avoid nutritional deficiencies. |
There is no doubt that the sleeve can be an excellent choice for some patients and it has obvious advantages compared with the other surgical options. However, the risks are not trivial and there is a tendency to regain weight over time.
If you would like to consider a sleeve, the key thing to remember is that you must stick to the nutritional and physical activity guidelines with which you will be provided.
The mistake made my many sleeve patients is that they think it’s an easy option because it really takes away the appetite and so doesn’t seem to need the same commitment to lifestyle change. This is completely wrong. The reduction of appetite due to changes in ghrelin may not be permanent and if you start eating large quantities again, you may stretch the remaining portion of your stomach. If this happens weight re-gain is inevitable.
REMEMBER: For long-term success the sleeve requires the same commitment to permanent lifestyle change as any other surgical weight loss procedure.
If you would like to learn more about the gastric sleeve procedure or to book an appointment, get in touch now or call 01 612 0551