
The gastric band has been in use for more than 25 years and has an unparalleled safety record. This is why we at Auralia believe the band should be the first-choice procedure for the majority of those with longstanding weight problems. But the band also has many other advantages:
From start to finish the staff were amazing and so reassuring. Had a gastric band fitted in March 2021 and honestly I’m sorry I didn’t do it years ago. Read More
I felt very informed and safe and well looked after. I had a breast augmentation in June 2018 and couldn’t be happier from start to finish. Read More
Couldn’t have dreamed of a better experience! Made me so comfortable and at ease. Couldn’t recommend Auralia enough I have never ever been happier! Read More
I couldn’t be happier with how my surgery went and I wouldn’t recommend anyone else I choose Auralia because of how helpful and friendly every single member of their team was to me. I couldn’t be happier with how my surgery went and I wouldn’t recommend anyone else! Read More
Not only life-changing has given me a newfound confidence in myself. I had two surgeries with the clinic. And everything from consultation, pre-op and post-op care was amazing. Read More
I couldn't be more pleased from my first consultation. I had a tummy tuck with muscle repair 8 weeks ago now and I couldn't be more pleased from my first consultation. Read More

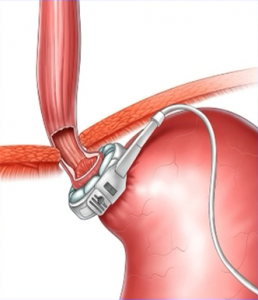
The band is essentially a hollow silicone structure which is fitted around the upper part of the stomach so as to form a small “pouch” above the band. Adding fluid (saline) through the access port, tightens the band and restricts the amount of food which can pass through into the stomach.
Click on the animation below to learn more.
Many people think the band is meant to stop them eating, but this is wrong.
The band actually works by producing satiety (a feeling of fulness), so you feel as though you have had enough even after eating only small amounts. How does this happen?
It happens because in the stomach wall beneath the band there are specialised nerve fibres (see images below).
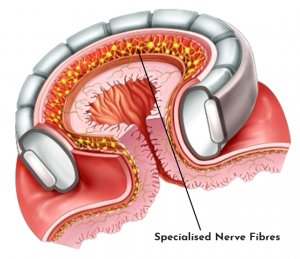
When food enters the pouch, the fibres are stimulated and send a message to the appetite centre in the brain – which produces a sensation of satiety. Feeling full after only small amounts of food means you will eat less – and lose weight.
 Overall weight loss
Overall weight lossGastric band weight loss results can vary and will depend on how well you follow the Band Rules – which includes eating slowly and choosing low-calorie options with the right texture.
But as a rough guide, you can expect to lose 50-60% of your excess weight over the first 2-years, although many patients go on to lose all of their excess weight. Here is an example:
In other words, you can expect to lose 2.5-3st
Do remember that this is an average weight loss – some will lose all their excess weight, whilst others may lose less than 50%.
Our experience suggests that at the time of the first band adjustment – usually around 5-weeks after surgery – average weight loss is around 1.5st (about 8% of starting weight). This is important, because we also know that good initial weight loss – even at this very early stage – predicts long-terms success.
Our clinical advisor (Dr David Ashton) and his colleagues, have published the only major study into gastric band surgery in the private sector, involving 2246 patients over a period of 8-years see here.
This shows that the band procedure is an extremely safe procedure – there were no fatalities and no serious complications – and the band delivered significant and durable weight loss. Complication rates overall were remarkably low.
Another study has carried out a 15-year follow-up on a group of 3,227 band patients. Average weight loss was 54.2% for these patients, again without any serious complications.
So all the evidence points to the band procedure being an extremely safe and effective weight loss option.
The gastric band operation is performed laparoscopically (also known as key-hole surgery) under a general anaesthetic.
The operation takes just 45 minutes and patients usually return home on the same day. Generally, 3-5 small incisions are made in the abdominal wall, through which surgical instruments can be passed. The band is then placed around the upper part of the stomach, about 2cm below where the oesophagus (gullet) joins the stomach. The procedure does not involve any cutting of the stomach or bowel and only a few sutures (stitches) are applied to keep the band in place. This means that the procedure is fully and relatively easily reversible.
Following gastric band surgery, you should spend the first few days resting at home, but light work is usually possible after that. Whilst some people return to work after a few days, we think it is prudent to take a full week away from work to recover. At the end of this period it should be quite safe to drive.
Incisions made during surgery are sutured and/or glued and the wounds normally heal within 10-14 days. The scars will tend to fade gradually, though some patients find it helpful to apply a silicone scar-reduction gel.
It’s important to start working with your band soon after surgery – you can start walking almost immediately. You should also stick closely to the nutritional guidelines with which you will be provided.
Remember – this is the beginning of a new chapter in your life!
As with any form of surgery, there are potential risks and complications associated with gastric band surgery, they include:
However, in the hands of an experienced bariatric team, these risks are remarkably low.
Typical side-effects immediately after surgery include:
However, most patients do not find the post-operative period difficult and these symptoms are usually short-lived. Pain is easily controlled with paracetamol and/or co-codamol.
Several longer-term complications can occur with gastric bands, but fortunately the most frequent of these are the ones which are most easily remedied – often without surgery. They include;
You can read more about long-term band complications here.
When the band is implanted, it will usually be completely empty of any fluid and will only be providing a very small amount of restriction around the stomach. Approximately 5 weeks after surgery, you can begin the process of having your band adjusted to control hunger, your food consumption and ultimately your weight loss.
A band fill / adjustment is when the level of restriction that the band exerts on the stomach is adjusted by injecting (also known as filling / inflating) the gastric band with a sterile saline solution to make the band tighter (narrowing the stomach and increasing restriction) or by removing existing saline to loosen the band (widening the stomach and reducing restriction). See the effect of three different fill volumes in the images below.

Adjustments are possible without the need for any additional surgery because the gastric band is connected via a tube to an access port placed just under the skin during the initial surgery.
Gastric band adjustments are made with a special (Huber) needle and syringe. For a skilled and experienced band clinician, the adjustment is generally straightforward and virtually painless. The exception to this is where the patient is very large or where the access port is lying in an awkward position. See my colleague Professor John Dixon performing a band adjustment:
Optimal adjustment
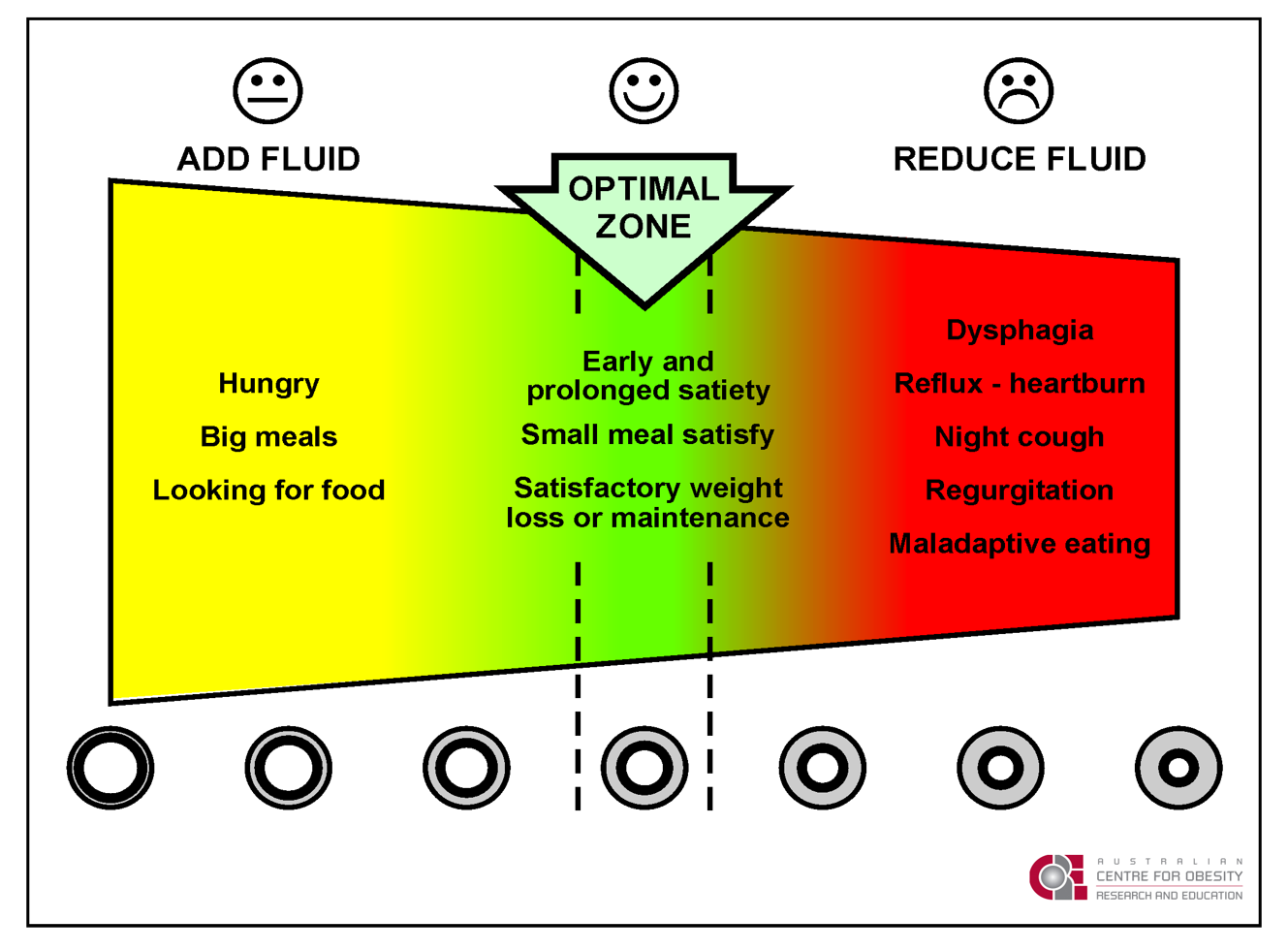
The band is optimally adjusted when the patient feels full with small amounts of food and is otherwise well. Adjusting the band to its optimum aperture size is a skill and is key to achieving good weight loss results. So it’s absolutely essential that your band provider can offer accurate and timely adjustments. Too little in the band and you will feel hungry and be looking for food – and weight loss will be minimal. Too much and you will be regurgitating food and engaging in “maladaptive eating”. This is where you are eating soft, calorie-rich foods such as cakes, crisps, chocolate (and cheesy wotsits!), because these are the only things you can tolerate.
See the chart below and make sure you are in the Green Zone:
Gastric banding has a major, often dramatic, impact on a wide variety of obesity associated conditions. Only a surgical intervention can provide such a sustained reduction in health risks, improve quality of life and protect against premature death and disability.
Some of the health benefits of band-associated weight loss are:
The above list is not exhaustive, but it accounts for the fact that band patients have – on average – a 60-70% lower risk of premature death when compared with their obese (non-banded) peers.
In summary, the band improves or resolves a range of obesity-associated weight problems, enhances social and psychological functioning and reduces the risk of premature death and disability. Not many procedures anywhere in medicine can offer such a remarkable list of benefits!
Let’s summarize the advantages and disadvantages of the gastric band:
| Advantages | Disadvantages |
| Very low risk | Requires regular attendance at clinic for adjustments |
| Fully reversible (preserves stomach and bowel) | Unlike sleeve or bypass the band does not reduce appetite hormones |
| Day-case procedure (usually) | Complications (though often minor) are relatively common) |
| Significant and durable weight loss | Health benefits are entirely dependent on weight-reduction |
| Major reductions in obesity-associated health risks | Can sometimes be a problem for those who do a lot of overseas travel |
| Low risk of vitamin and mineral deficiency | Experience of the surgeon directly related to the risk of long-term complications |
There are alot of rumours about Gastric Bands – here we dispel some of the myths surrounding them.
The myth here is that you can’t have fizzy drinks after a band because it will cause bloating and may “stretch” the stomach. You can find advice of this kind even on NHS websites. In fact, as long as they don’t cause any discomfort, zero calorie fizzy drinks are perfectly fine. I have lots of successful band patients who enjoy diet coke (as do I) and other zero calorie drinks without any difficulty.

This is a remarkably durable myth, which even bariatric surgeons seem to believe. But the evidence is quite clear – sweet eaters who have bands do just as well as those who don’t generally eat sweets. In fact there is even a study which showed that NOT eating sweets increased the risk of failure with the band!”. Of course, trying to define a “sweet eater” is not always easy”. Clearly, if you have a band and you eat 1kg of chocolate every day, you’ll fail – but you will fail with any procedure. But there is nothing specific about the band – or about sweets – that spells failure. If you have a band and all you eat is a bar of your favourite chocolate every day, you will lose weight. In the end, what matters is calories rather than specific foods.

The idea that you shouldn’t eat and drink at the same time is another old chestnut, based on a an entirely outdated idea of exactly how the band works. The belief is that food needs to stay in the pouch above the band in order to give the feeling of fullness (satiety) and that drinking and eating at the same time will “wash” the food through the band and into the stomach. This is not the case.
In fact when food passes into the pouch, there is almost no delay at all before it passes through the band into the stomach. The sensation of fullness is created by special nerves in the upper part of the stomach and is not the result of any significant delay in the pouch emptying. So drinking whilst eating makes no difference and does no harm.
However, you should bear in mind that because the pouch is small (about 10% of the total stomach volume) you should only drink very small volumes – and slowly – whilst eating. If you drink larger volumes quickly you will have pain and you may regurgitate the fluid (not too great for your partner!).

The idea seems to be that because of changes in cabin pressure whilst flying, the air in the band will expand and cause a tightening of the device around the stomach. This might be true if the gastric band is filled (adjusted) with air, but it isn’t. A band is filled with a sterile salt (0.9% saline) solution and there should be no air at all within the system. So nothing happens to the band.
It is quite true that band patients often say that when they fly (especially long-haul) the band feels tighter. But this is because air in the stomach expands due to relative cabin decompression. In other words, it is the stomach that expands against the band. Usually excess air is passed or absorbed within 24-hours of being back on the ground at normal atmospheric pressure.

It’s perfectly OK to get pregnant with a gastric band in place. In fact, many band patients have a condition called Polycystic Ovarian Syndrome (PCOS) which is strongly associated with weight gain and infertility. When they lose weight with the band, they quite often find themselves fertile again – and sometimes become pregnant quite quickly. This may even be why they wanted to have a band in the first place.
We have a well worked out protocol for managing the band during pregnancy. However, we recommend that if you are planning to start a family it’s a good idea to wait until you have achieved significant weight loss. This is because the closer your weight is to normal when you are pregnant, the lower the risks for both you and the baby. For example, losing weight before becoming pregnant will dramatically reduce your risk of developing gestational diabetes and blood- pressure problems.

Wrong again. It’s possible that this idea stems from the practice of putting patients on a “liver reducing diet” (usually soft or semi-liquid) for a couple of weeks before the band surgery. Some surgeons feel this makes the procedure technically easier to perform, though other think this is irrelevant. Most experts recommend a post-operative diet of liquids, followed by pureed foods. But from then onwards, it’s important to eat a normal, balanced diet consisting mainly of lean meats, fish, wholegrains, fruit and vegetables. No more mush!

It is widely believed that a gastric band causes reflux (heartburn) or makes existing heartburn worse. This is generally not the case. In fact there is good scientific evidence that gastric banding actually improves or completely cures reflux. The exception to this is when a band is over-tightened when reflux is both common and distressing. ANY band patient with persistent reflux should have the device completed aspirated (emptied).

A unique feature of the band – one too easily forgotten by enthusiasts for procedures such as bypass and sleeve – is that the gastric band is entirely reversible. It does not require any permanent re-configuration of the stomach or bowel, unlike more disruptive options such as sleeve and bypass. This means that if you needed to have a band removed and wanted to consider another type of bariatric procedure, this is entirely feasible. In fact, conversion to a bypass or sleeve can often be done at the same time as the band removal.

This isn’t the case. In general, major vitamin and mineral (micronutrient) deficiencies are very uncommon after gastric banding, unlike gastric bypass and sleeve. Gastric bypass in particular, requires intensive and lifelong vitamin and mineral supplements. We recommend that gastric band patients take a daily vitamin and mineral supplement, but one of the commercially available options is perfectly adequate.

The only metal (steel) part of the gastric band is in the access port, which is encased within a silicone shell. This does not usually set walk-through metal detector scanners off, though a hand-held wand detector may possibly identify it. The newer, so-called full body scanners make a surface map image. Nothing internal can be seen. If you lose an excessive amount of weight, the access port may be somewhat superficial and a bump may appear on the body scan. Other than this cause for celebration, no one will know you have a band!

Not true. It’s actually perfectly safe to undergo magnetic resonance imaging (MRI) after having a gastric band implanted.
Call 01 612 0551 for further information or visit the contact page.